Case Report
Ukrainian Neurosurgical Journal. 2024;30(4):64-67
https://doi.org/10.25305/unj.311488
1 Department of Neurosurgery, Istinye University Faculty of Medicine, Liv Hospital Vadistanbul, Istanbul, Türkiye
2 Department of Neurosurgery, İstanbul Medeniyet University, Prof. Dr. Süleyman Yalçın City Hospital, Istanbul, Türkiye
3 Department of Neurosurgery, University of Health Sciences, Prof. Dr. Cemil Taşcıoğlu City Hospital, Istanbul, Türkiye
Received: 13 September 2024
Accepted: 11 October 2024
Address for correspondence:
Ozan Baskurt, M.D., Department of Neurosurgery, Istinye University Faculty of Medicine, Emirgan mah. Camlar sok. No:23 Cam Palas Apt Daire:6 Sariyer, Istanbul, Türkiye, e-mail: ozanbskrt@gmail.com
Multisutural synostosis, characterized by the fusion of multiple cranial sutures without a clear underlying syndrome, represents a rare subtype of craniosynostosis. Particularly uncommon is the simultaneous fusion of the sagittal, metopic, and bilateral coronal sutures. This report details the case of a 50-month-old boy, who had an abnormal head shape due to the simultaneous fusion of four sutures. The closure of the sagittal, metopic, and bilateral coronal sutures has led to a distinct head shape marked by flattening of the forehead and anterior skull, contrasting with the typical Mercedes-Benz pattern observed in craniosynostosis cases. Surgical intervention involved osteotomy with symmetrical barrel staves in the parietal and frontal regions, resulting in improved forehead contour.
Key Words: brachicephaly; craniosynostosis; multisutural craniosynostosis; nonsyndromic craniosynostosis; scaphocephaly; trigonocephaly
Abbreviations: C - coronal, L - lambdoid, M - metopic, S – sagittal
Introduction
Craniosynostosis refers to the premature fusion of one or more cranial sutures, resulting in an abnormal head shape [1]. Typically, it manifests as an isolated fusion affecting a single suture and is not commonly associated with an identifiable genetic syndrome [2]. In contrast, syndromic synostoses, though less prevalent, often involve multiple sutures, including at least both coronal (C) sutures [3].
Apart from these syndromic cases, a small subset of patients exhibits a complex pattern of synostosis without an easily identifiable underlying syndrome. Involvement of the metopic (M) and sagittal (S) sutures, followed by the S and bilateral lambdoid (2L) sutures, represents the most common types of this multisutural, nonsyndromic craniosynostosis [4]. Simultaneous fusion of the S, M, and bilateral coronal (2C) sutures is exceptionally rare.
This report presents a case of complex nonsyndromic craniosynostosis where four sutures (S, M and 2C sutures) were fused simultaneously and its surgical management.
Case Presentation
A 50-month-old boy was admitted to the neurosurgery department with an abnormally shaped head since early infancy. He had an uneventful delivery at 30 weeks via C-section due to a breech-presenting twin. After lying in an incubator for 3 weeks, he always lagged behind his peers in terms of head circumference, height and weight. According to the parents, his development was normal within the typical developmental milestones. His head circumference was between the 10th and 25th percentile for his age group. The patient was examined for the syndrome before admission to our clinic, but no pathology was found.
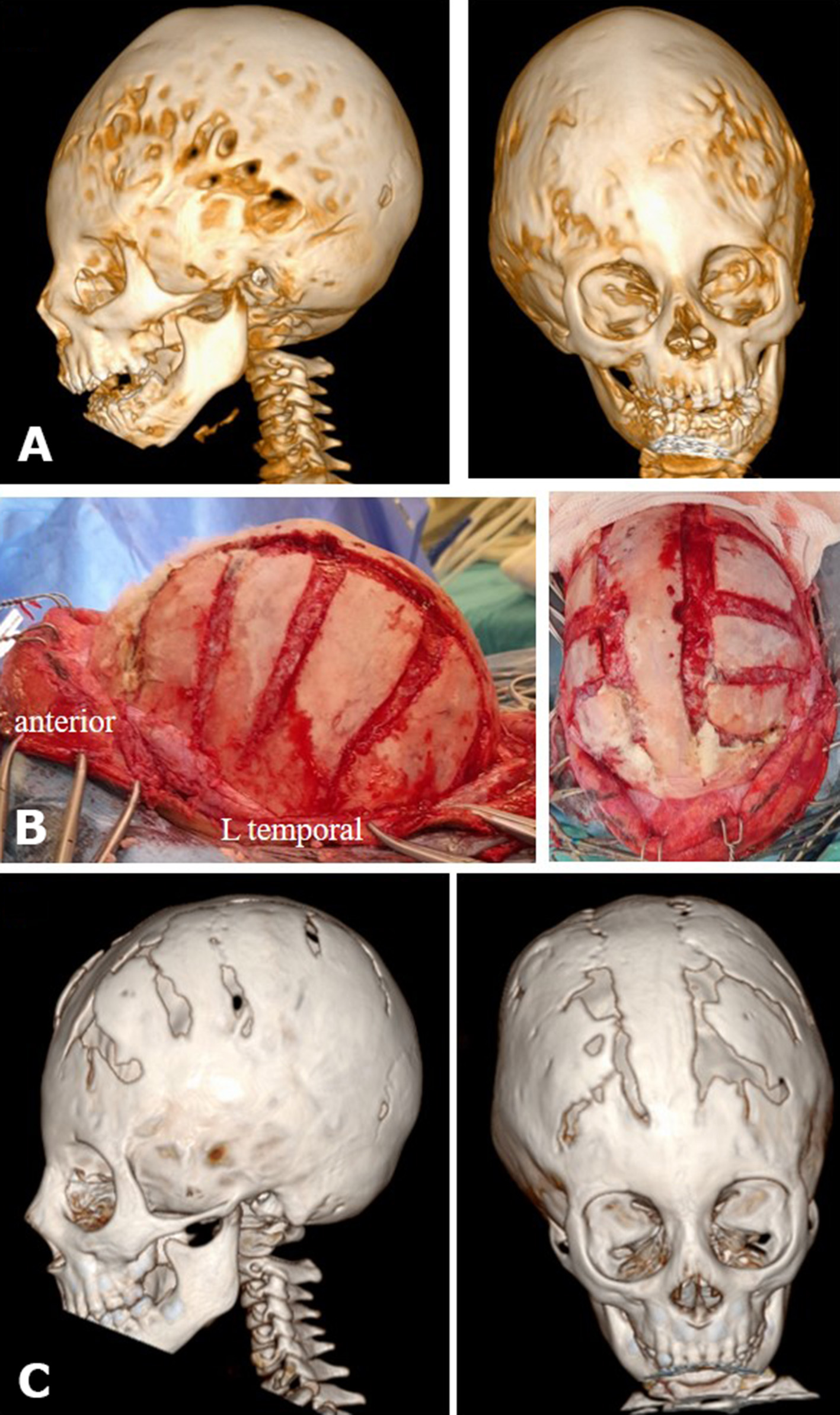
He presented with an unusual cranial shape characterized by distinctive frontal flattening of the cranium as the main feature of this rare form of craniosynostosis. Three-dimensional computed tomography revealed the fusion of the S, M, and 2C sutures. Radiological sign of increased intracranial pressure was also noted via the copper beaten skull appearance (Fig. 1A). Fundoscopic examination was normal.
The child underwent surgery. After a bicoronal skin incision, bilateral paramedian parietal bony incision using a high speed craniotome along the fused S suture was made. The middline S bone left in place. The craniotomy was extended beyond the closed cranial suture along the M suture. Then bilateral barrel-stave osteotomies were performed bilaterally and extended to the contiguous frontal bone with bilateral removal of fused C sutures (Fig. 1B). The postoperative course was uneventful. Postoperative assessments noted improvement in forehead flattening, with further enhancement observed fifteen months post-surgery. Radiologic evaluation showed resolution of the increased intracranial pressure on the cranial bone with widened biparietal diameter (Fig. 1C).
Fig. 1. A - 3D head computed tomography, lateral and anterior views; fusion of the bilateral coronal, metopic, and sagittal sutures with signs of increased intracranial pressure with copper beaten appearance.
B - Peroperative image, lateral and superior view; osteotomy with symmetrical barrel staves in the parietal and frontal regions.
C - 3D head computed tomography, lateral and anteior views; postoperative 15th month, showing improved flattening of the forehead, resolution of the copper beaten appearance with a widened biparietal diameter.
Discussion
In about 85% of cases, craniosynostosis is limited to a single suture. The anatomical classification is based on the involved suture [5]. The most common form, with a prevalence of 45% to 50% of all nonsyndromic craniosynostosis, is S synostosis. Recent epidemiologic studies have shown that about 25% of all patients have M synostosis, which is the second most common form [3]. C (unilateral or bilateral) synostosis accounts for 17%, while L synostosis is thought to account for 1-5% of all nonsyndromic craniosynostosis [6].
Approximately 15% of cases are syndromic synostoses, usually involving multiple sutures, including at least 2C sutures [3]. When the S+2C sutures are fused, the membranous bones of the calvarium expand between the sutures, giving the appearance of a cloverleaf as in Kleeblattschädel syndrome; or a high forward tilted head in the form of acrocephaly as observed in Apert syndrome. In craniosynostosis with 2C+L sutures, the forehead recedes, resulting in an upturned, posteriorly declined head and a pointed skull shape, which is associated with compensatory hypergrowth of the bregmatic fontanel in the form of oxycephaly as in Crouzon syndrome [7-9].
Aside from these syndromic craniosynostoses, there is a small subgroup of patients with a multisutural synostosis pattern in whom the underlying syndrome is not readily apparent. Czerwinski et al. retrospectively analyzed 858 patients who underwent craniosynostosis over an 18-year period and found only 37 (4%) cases of nonsyndromic multisutural craniosynostosis [4]. In this study, M+S suture synostosis (10 of 37), followed by 2L+S suture synostosis (7 of 37) were most commonly found [4]. In another study, S+L synostosis was found to be the most commonly observed form of nonsyndromic craniosynostosis (6 in 20 cases of nonsyndromic multisutural craniosynostosis) [6]. The simultaneous involvement of the S+M+2C sutures is exceedingly rare. Czerwinski et al. reported only three cases, while Boulet et al. identified only one case in their craniosynostosis series [4, 5].
This rare case of multiple suture synostosis is particular in terms of the characteristic head shape. This is basically the contrary of the shape that occurs in case of Mercedes-Benz pattern craniosynostosis in which the fusion of S+2L sutures led to a turricephaly in association with scaphocephaly. The main cranial characteristic feature of Mercedes-Benz pattern craniosynostosis is a frontal bossing associated with a posterior parietal flattening (S+2L: anterior oxycephaly with posterior flattening: “Mercedes-Benz pattern”) [1, 10, 11]. It is important to note that the M suture is naturally a continuum of the S suture beyond the anterior fontanel [12] . Therefore in our presented case, as a contrary of Mercedes-Benz pattern, the flattening was frontal and a relative backward prominence of that head shape as the result of S and M synostosis with closed 2C sutures [4-5] (S+M+2C: posterior oxycephaly with anterior flattening: “Scapho-trigo-brachicephaly").
Conclusion
We herein report a rare case of nonsyndromic, multisutural cranisynostosis involving the S+M+2C sutures, scapho-trigo-brachicephaly; and a characteristic flattening of the forehead, as a contrary of Mercedes-Benz pattern craniosynostosis.
Disclosure
Acknowledgements:
None.
Declaration of Interests:
The authors have no relevant financial or non-financial interests to disclose.
Funding:
The authors did not receive support from any organization for the submitted work.
Consent:
Written informed consent was obtained from the legally authorized representative of the patient for publication of this case report and any accompanying images.
Ethical statement:
The need for ethical approval was waived by Istinye University Ethics Committee.
Data Availability:
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Authors’ Contribution
Study conception and design: OB, TH. Data collection: OB, HŞÇ. Analysis and interpretation of results: OB, HŞÇ. Draft manuscript preparation: OB, HŞÇ, EU. Critical revision of the article: TH. Study supervision: TH. All authors (OB, HŞÇ, EU, TH) reviewed the results and approved the final version of the manuscript.
References
1.Kajdic N, Spazzapan P, Velnar T. Craniosynostosis - Recognition, clinical characteristics, and treatment. Bosn J Basic Med Sci. 2018 May 20;18(2):110-116. https://doi.org/10.17305/bjbms.2017.2083
2.Xue AS, Buchanan EP, Hollier LH Jr. Update in Management of Craniosynostosis. Plast Reconstr Surg. 2022 Jun 1;149(6):1209e-1223e. https://doi.org/10.1097/PRS.0000000000009046
3.Yilmaz E, Mihci E, Nur B, Alper ÖM, Taçoy Ş. Recent Advances in Craniosynostosis. Pediatr Neurol. 2019 Oct;99:7-15. https://doi.org/10.1016/j.pediatrneurol.2019.01.018
4.Czerwinski M, Kolar JC, Fearon JA. Complex craniosynostosis. Plast Reconstr Surg. 2011 Oct;128(4):955-961. https://doi.org/10.1097/PRS.0b013e3182268ca6
5.Nagaraja S, Anslow P, Winter B. Craniosynostosis. Clin Radiol. 2013 Mar;68(3):284-92. https://doi.org/10.1016/j.crad.2012.07.005
6.Boulet SL, Rasmussen SA, Honein MA. A population-based study of craniosynostosis in metropolitan Atlanta, 1989-2003. Am J Med Genet A. 2008 Apr 15;146A(8):984-91. https://doi.org/10.1002/ajmg.a.32208
7.Vinchon M, Guerreschi P, Karnoub MA, Wolber A. Synostosis of the lambdoid suture: a spectrum. Childs Nerv Syst. 2021 Jun;37(6):1991-2000. https://doi.org/10.1007/s00381-020-05003-9
8.Blaser SI. Abnormal skull shape. Pediatr Radiol. 2008 Jun;38 Suppl 3:S488-96. https://doi.org/10.1007/s00247-008-0867-0
9.Bennis Y, Wolber A, Vinchon M, Belkhou A, Duquennoy-Martinot V, Guerreschi P. Les craniosténoses non syndromiques [Non syndromic craniosynostosis]. Ann Chir Plast Esthet. 2016 Oct;61(5):389-407. French. https://doi.org/10.1016/j.anplas.2016.07.004
10.Balestrino A, Secci F, Piatelli G, Morana G, Pavanello M, Pacetti M, Cama A, Consales A. Pure Bilateral Lambdoid and Posterior Sagittal Synostosis (Mercedes-Benz Syndrome): Case Report and Literature Review. World Neurosurg. 2019 Aug;128:77-82. https://doi.org/10.1016/j.wneu.2019.04.117
11.Dinis J, Junn A, Lu X, Lopez J, Persing J. Aberrant Morphologic Patterning of Combined Sagittal and Metopic Craniosynostosis. J Craniofac Surg. 2021 Sep 1;32(6):2184-2185. https://doi.org/10.1097/SCS.0000000000007676
12.Pontell ME, Barrero CE, Wagner CS, Salinero LK, Swanson JW, Taylor JA, Bartlett SP. Oxycephaly-systematic review, case presentation, and diagnostic clarification. Childs Nerv Syst. 2023 Nov;39(11):3041-3049. https://doi.org/10.1007/s00381-023-06048-2